

Hesperian Health Guides
Chapter 55: Examples of Community-Directed Programs
Contents
- 1 1. PROJIMO — RURAL MEXICO
- 2 2. LOS PARGOS-URBAN MEXICO
- 3 3. CENTRE FOR THE REHABILITATION OF THE PARALYSED (CRP)— BANGLADESH
- 4 4. ORGANIZATION OF DISABLED REVOLUTIONARIES — NICARAGUA
- 5 5. COMMUNITY-DIRECTED REHABILITATION DEVELOPMENT — PAKISTAN
- 6 6. HANDICAP INTERNATIONAL ARTIFICIAL LIMB PROGRAM—THAILAND/KAMPUCHEA
1. PROJIMO — RURAL MEXICO
Project PROJIMO is a rural rehabilitation program in western Mexico, run by villagers with disabilities, to serve children with disabilities and their families. It was started in 1982 by village health workers with disabilities from an older community-based health program (Project Piaxtla).
PROJIMO’s goal is to help children with disabilities and their families become more self-reliant. It aims to provide low-cost, high-quality services to poor families who cannot obtain or afford services elsewhere.
The PROJIMO team provides a wide range of rehabilitation activities and equipment. These include: family counseling and training, therapy, work and skills training, brace making, artificial limbs, wheelchair making, special seating, and therapeutic aids. PROJIMO is based in one small village but serves children and their families from neighboring towns and villages, and even from the closest cities (over 100 miles away). Local villagers cooperate by taking visiting children with disabilities and their families into their homes. Schoolchildren help make the playground for all children and toys for children with disabilities.

PROJIMO DIFFERS FROM MANY REHABILITATION PROGRAMS IN A NUMBER OF WAYS:
- Community control.Unlike many “community-based” programs, which are designed and run by outsiders, PROJIMO is run and controlled by local villagers with disabilities.
- De-professionalization. The village team, although they have mastered many professional skills, is made up of people with disabilities with an average education of 3 years of primary school. Their training has been mostly of the non-formal, learn-by-doing type. There are no titled professionals on the PROJIMO staff. However, therapists, brace makers, limb makers, and other professionals are invited for short visits to teach rather than to practice their skills.
- Equality between service providers and receivers. When asked how many “workers” they have, the PROJIMO team has no easy answer. This is because there is no clear line between those who provide services and those who receive them. Visiting young people with disabilities and their families are invited to help in whatever way they can. Most of the PROJIMO workers first came for rehabilitation themselves. They began to help in different ways, decided to stay, and gradually became team members.
- Self-government through group process. The PROJIMO team has been trying to develop an approach to planning, organization, and decision-making in which all participants take part. They are trying to free themselves from the typical "boss-servant" work relationship and form more of a work partnership. The group elects its coordinators on a one-month rotating basis so that everyone has a turn. This leads to a lot of inefficiency and confusion, but to a much more democratic group process.
- Modest earnings. The PROJIMO team believes that they should work for the same low pay as that of the farming and laboring families they serve. They see that the high pay demanded by professionals and technicians is one reason that the children of the poor often cannot get the therapy and aids they need.
 |
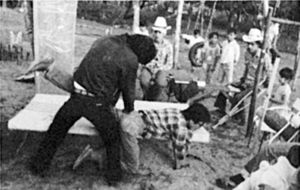
|
| Roberto Fajardo and Mari Picos, two of the leaders of PROJIMO, evaluate a child’s developmental level. Both Roberto and Mari first came for rehabilitation, then stayed in order to help others. |
 |
Most of the training of the PROJIMO team members is through guided “learning by doing.” Here, PROJIMO workers practice exercises under the guidance of a visiting physiotherapist. Parents, children, and anyone who wants to learn are welcome. |
| 6. Unity with all who are marginalized. The PROJIMO team sees society’s unfair attitudes toward people with disabilities as only one aspect of an unjust social structure. They feel that people with disabilities should join in solidarity with all who are rejected, misjudged, exploited, or not treated as equals. This feeling has led the team to become more self-critical and to seek greater equality for women within their own group. Thus the PROJIMO team views its role not only as one of helping children with disabilities and their families gain power, but as part of the larger struggle for social change and liberation of all who are "on the bottom". |
| 7. Grassroots multiplying effect. The PROJIMO approach has been spreading in various ways. Locally, families of children with disabilities in a number of towns and villages have begun to organize, build playgrounds, and form their own special education programs, as more or less “satellites” of PROJIMO. PROJIMO has also invited visitors from rehabilitation and community health programs in other parts of Mexico and Latin America to visit and take ideas back with them. Some programs have sent representatives with disabilities to work and learn at PROJIMO for several months so they can start similar programs in their own area. |
2. LOS PARGOS-URBAN MEXICO
Los Pargos is an organization of families of children with disabilities in Mazatlán, a city on the west coast of Mexico. The program was started privately by Teresa Páez, a local social worker. While she was working in a public hospital, Teresa became concerned that although children with disabilities were given basic medical treatment, they received almost no rehabilitation. Most did not go to school because of non-acceptance by teachers, difficulties in transportation, or overprotection by parents.
Teresa began by bringing a group of concerned parents together, and they invited others. Today Los Pargos includes about 60 families of children with disabilities, and it continues to grow.
Los Pargos has set up its own special education program and has convinced the local university authorities to make space available in a local prep school after school hours. Some of the teachers, who are volunteers, are also people with disabilities. This makes them good role models for the children.

The word “Pargos” is the name of a large, colorful fish! The children picked the name. It is perhaps appropriate, since much of the money for running the program and transporting the children comes from fish scales! On weekends the children and their parents visit the beach where fishermen dock their small boats and clean their fish for the market. The group collects the large fish scales, which they clean, bleach, color, and use to make artificial flowers. The children and parents set the flowers in attractive bouquets and designs together with small seashells, seaweed, and other dried sea life. In the tourist city of Mazatlán, selling the flowers has become a good business. When we last visited Los Pargos, parents and children were working very hard to fill a rush order for 2000 bouquets!
Los Pargos, located about 100 miles from PROJIMO, often takes groups of “parguitos” (children with disabilities) to PROJIMO for rehabilitation services that they have trouble getting in the city. Also, their visit to PROJIMO is an adventure into the country for these city children and their parents.
 |
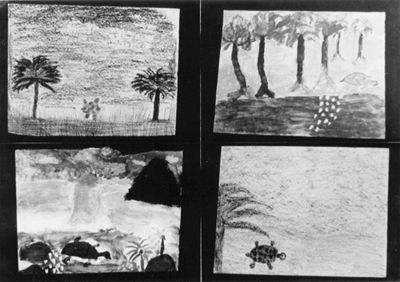 |
| One of the children of Los Pargos waters a young tree—part of an orchard the parents and children are planting together. | Four pictures of sea turtles, painted by Los Pargos children, as a part of their “Save the Turtles” campaign. |
One of the goals of Los Pargos is to convince the government, the public schools, and society in general to accept, respect, provide opportunities, and help meet the needs of children with disabilities. Some things are changing, but slowly. As one of the parents explains, “The best way to get something done is to do it ourselves!”
The idea of Los Pargos has begun to spread to other communities. Families of children with disabilities in Culiacán, the next biggest city to the north, are trying to organize a similar program. The key to success seems to be a few persons with energy, commitment, and an ability to get people working together.
3. CENTRE FOR THE REHABILITATION OF THE PARALYSED (CRP)— BANGLADESH
Located in the capital Dhaka, CRP is run by a local team, with the help of a British physiotherapist. Four of the staff members have spinal cord injuries themselves.
The CRP provides short- and long-term “participatory rehabilitation” to people with paralysis. Almost from the day of arrival, newly paralyzed persons begin to do jobs to help the Centre bring in some income. Those who must lie on stretcher trolleys (wheeled cots) work on jobs ranging from making paper bags to be sold in the local marketplace, to welding and painting of orthopedic equipment. The group produces orthopedic and hospital equipment, not only for those it serves directly, but also for sale in hospitals and in the community.
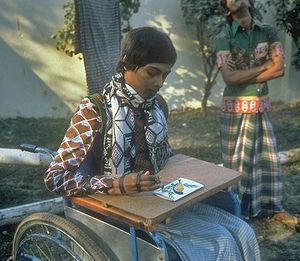 |
Madhab, a person with quadriplegia who has been employed as the Centre’s counselor since 1980, paints by means of a simple hand splint. Workers with disabilities print his paintings as greeting cards and sell them to bring in money. Madhab is responsible for the education program. He supervises those who read and write, who teach classes to those who do not. |
CRP teaches practical skills through “learning by doing.” The work that participants do not only brings in money for the program, but also teaches them ways to earn money after they return home. Skills learned are mostly those that will let persons have their own small home business—a roadside stand, sewing and tailoring, weaving, welding, and metalwork.
CRP has developed a wide range of low-cost orthopedic and rehabilitation equipment adapted to the needs and lifestyle of local villagers. Examples are ground level wheelchairs, or ‘trolleys’, for those who cook and eat on the floor, and simple metal frame beds that can be easily lowered to near ground level for easy transfer into the low trolleys.
 |
 |
| Badd, a person with quadriplegia, pedals a CRP made “exercycle” while Delwar, a person with paralysis from tuberculosis of the spine, practices walking. | A worker in the CRP-made wheelchair makes a bedside stand to be sold to a local hospital. |
Although CRP is much loved by people with disabilities and their families, it has suffered attacks —sometimes physical—from opposition groups. (Many successful community-directed programs have faced similar diffculties—partly because they provide friendly, flexible, effective care that differs so much from the services provided by many large institutions.)
The Centre for the Rehabilitation of the Paralysed is financed mainly from outside grants and partly from the sale of its products.
For more information on this center and its equipment, see "Padding and cushions for lying", "Local Funding", and “Adjustable Beds”. Also see its website: www.crp-bangladesh.org.
4. ORGANIZATION OF DISABLED REVOLUTIONARIES — NICARAGUA
 |
 |
 |
| The ORD team of workers produced its own high-quality metal tubing wheelchairs, adapted for rough ground at a cost far lower than standard commercial wheelchairs. |
The Organization of Disabled Revolutionaries (ORD) was started after Nicaragua’s liberation from the Somoza dictatorship, by a group of young persons with paralysis due to spinal cord injuries. Some had been boys of 13, 14 or 15 years old when they first joined the struggle against Somoza.
ORD was begun because of concern for a common need: wheelchairs. With the increase in people with disabilities from the war, the lack of a local wheelchair factory, and the difficulties of importing wheelchairs due to the United States’ embargo, the shortage was severe.
Two young North Americans who both have spinal cord injuries, one a peer counselor for people with disabilities and the other a wheelchair designer and engineer, helped ORD organize and set up a small wheelchair factory.
Although ORD started with wheelchairs, it grew to become a group that represented and stood up for the rights of all people with disabilities. It pressured the Health Ministry to respond more to people with disabilities and their needs. The government, which tried to represent the people much more than most governments, responded well. It allowed ORD time for short educational programs on public radio and television. And it agreed to help pay the cost of wheelchairs made by ORD for families too poor to pay. ORD was in close communication with the head of rehabilitation for the nation. In this way, the organization had some voice in national policy making.
These are some of the advantages experienced by a community-directed program in a country with a revolutionary popular government. On the other hand, ORD suffered from the embargo and other difficulties imposed by the United States government. At times, the wheelchair production almost stopped for lack of metal tubing, bearings, and other basic materials.

ORD had a far-reaching influence. It helped organize groups of people with disabilities in other parts of Nicaragua. Also, members have helped conduct training workshops in Central American and Caribbean countries to teach representatives from other groups how to make wheelchairs.
5. COMMUNITY-DIRECTED REHABILITATION DEVELOPMENT — PAKISTAN
The program began in Peshawar in the Northwest Frontier Province of Pakistan as a small play group for 8 mentally handicapped children. In 1978 the 3 Pakistani staff were joined by a Welsh special education teacher and her husband. During the next 7 years the play group grew to become a community rehabilitation and resource center with daily participation of 70 physically and 40 mentally and multiply disabled children.
 |
 |
| Splinting a leg to straighten a knee contracture. | Helping a child begin to learn to move. |
Local staff persons are trained by the few professionals in special education, rehabilitation therapy, brace making, parent counseling, and planning services.
An important part of the program is the Community Rehabilitation Development Project. The big, largely rural area surrounding Peshawar is very underserved. To accomplish as much as possible with limited resources, children with disabilities in towns were considered first. Volunteer college students went door-to-door to find and bring together parents and relatives of children with disabilities. Public meetings were held and an Association was formed in each town with the aim of starting rehabilitation activities. People (sometimes young people with disabilities) were chosen and sent to learn basic skills at the Peshawar center. Meanwhile, the Association committee raised funds and found a place that could serve as a modest rehabilitation center.
Although the parent program has had UNICEF and other outside funding, the neighborhood rehabilitation centers have mostly been funded locally, some with a government subsidy. Management is entirely in the hands of local people.
In addition to providing daily special education and rehabilitation therapy, the neighborhood centers act as a resource within their districts. They distribute advice, pamphlets, and books to families for home rehabilitation. Where possible, going to the same schools as children without disabilities is encouraged.
12-minute radio broadcasts about home rehabilitation started in 1984. (The scripts for these, which are excellent, are available at the website of Disability World.) An article on handicrafts by which disabled young people can contribute to their family’s income is at independentliving.org. (See examples.)
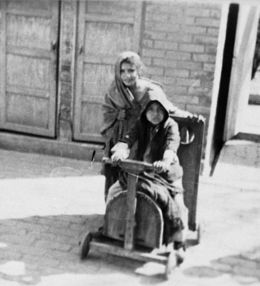 |
| Going for a ride. |
Also available is an excellent book by Christine Miles, called Special Education for Mentally Handicapped Pupils: A Teaching Manual. It points out the importance of re-thinking special education to meet local needs and customs in developing countries.
M. Miles, Christine’s husband, has also written many excellent and critical papers on rehabilitation efforts — and problems — in developing countries (see www.independentliving.org).
The Peshawar program has succeeded in promoting community-directed rehabilitation activities in much of the Northwest Frontier through organizing an already motivated group (parents of children with disabilities).
One of their keys to success is to “Do the easy thing first!”
6. HANDICAP INTERNATIONAL ARTIFICIAL LIMB PROGRAM—THAILAND/KAMPUCHEA
It is estimated that in the last 8 years of the war in Kampuchea (Cambodia) more than 12,000 men, women, and children have lost their legs from stepping on land mines. A lot of the injured are evacuated for hospital care to a large refugee camp, called Khao-i-dang, close to the Thai border.
At first the hospital had no way of making or obtaining artificial limbs. For this reason a French relief agency (at that time SOS, or Enfants Sans Frontières, now Handicap International) began making low-cost artificial legs.
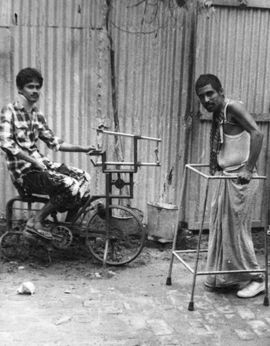
The workers in the large workshop are almost all refugees with amputations. Some start learning by helping to make their own leg.
The team (run by French relief workers, some of whom are professional limb makers) has developed different models of very low-cost limbs using local materials. This bamboo limb is one example.
Bamboo is in fact the main building material for the shop itself, the rehabilitation center next door, and for most of the beds, aids, and equipment. The rehabilitation playground (which served as a model tor PROJIMO) is made completely of bamboo.
One of the most outstanding features of the program is the way it has spread to other areas. Many of the workers with amputations trained in Khao-idang have gone back into Kampuchea and opened small artificial limb shops. The program therefore trains the workers not only in the technology of limb making, but also in basic management. Some of the 15 satellite shops now have teams of several people with amputations working in them. The most remote shops are run in makeshift shelters deep in the forest near the fighting.
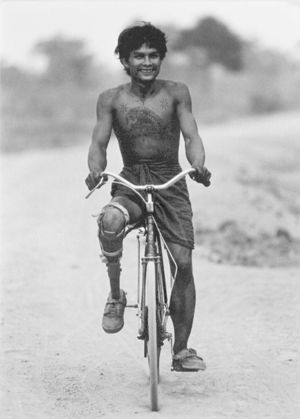
The spirit of hard work and friendship in shops run by people with amputations does much to help recent people who have recently experienced amputation to cope with the loss of their limbs and get back into the adventure of survival.

Photos from the OHI Limb Program, Thailand
 |
 |
 |
 |