

Hesperian Health Guides
Secondary Disabilities to Look for with Paralysis
HealthWiki > Disabled Village Children > Chapter 7: Paralysis > Secondary Disabilities to Look for with Paralysis
By secondary problems, we mean further disabilities or complications that can appear after, and because of, the original disability.
Contents
TYPICAL CONTRACTURES IN PARALYSIS
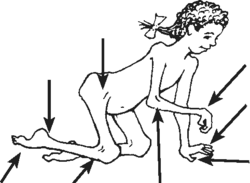
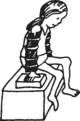
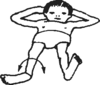
A child with paralysis who crawls around like this and never straightens her legs will gradually develop contractures so that her hips, knees, and ankles can no longer be straightened.
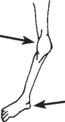
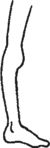
TYPICAL DEFORMITIES
OF ANKLE AND FOOT
OF ANKLE AND FOOT
 |
|||
| bending down at ankle (tiptoe) contracture) | bending down at mid-foot | bending out at ankle | bending in at ankle |
CONTRACTURES OF JOINTS
A contracture is a shortening of muscles and tendons (cords) so that the full range of limb movement is prevented.
Unless preventive steps are taken, joint contractures will form in many paralyzed children. Once formed, often they must be corrected before braces can be fitted and walking is possible. correction of advanced contractures, whether through exercises, casts, or surgery (or a combination), is costly, takes time and causes discomfort. Therefore early prevention of contractures is very important.
A full discussion of contractures, their causes, prevention, and treatment is in the next chapter (Chapter 8). Methods and aids for correcting contractures are described in Chapter 59.
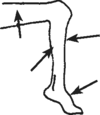
OTHER COMMON DEFORMITIES
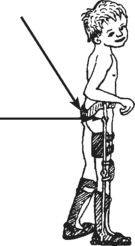
Weight bearing (supporting the body’s weight) on weak joints can cause deformities, including:
OVER-STRETCHED JOINTS
 bending
out at knee foot out of line with knee(when knee points forward, foot points to the side)
|
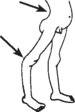 swayback
back-knee
|
DISLOCATIONS
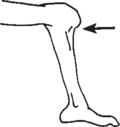 | partly dislocated knee | |
| partly dislocated foot |
WARNING! Dislocations like these are sometimes caused by stretching contractures incorrectly.
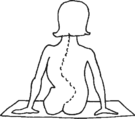
| SPINAL CURVE | ||
| Minor curve of spine can be caused by tilted hips,as a result of a short leg. | 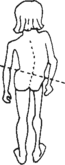 |
More serious curve of the spine is caused by muscle weakness of the back or body muscles. The curve can become so severe that it endangers life by leaving too little room for the lungs and heart. |
| a severely paralysed child | |
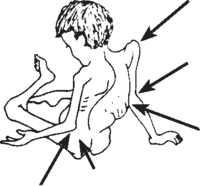 dislocated shoulder
elbow bent backward
apparent hunchback from bulge of ribs
elbow contracture
dislocated hip |
At first, the spinal curve straightens when the child is positioned better. But in time the curve becomes more fixed (will not straighten any more). For information on spinal curves, see Chapter 20. |
To prevent complications in a child with paralysis:
- Prevent contractures and deformities by beginning appropriate range-of-motion exercises as soon as the paralysis appears.
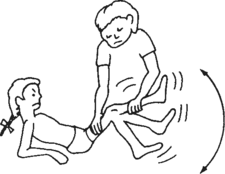
- At the first sign of a joint contracture, do stretching exercises 2 or 3 times a day — every day.
Stretching exercises work better if you stretch the joint firmly and continuously for a few moments,
... instead of ‘pumping’ the limb back and forth.
For more details, see “Contractures,” Chapter 8.
- Evaluate the child’s needs regularly, and change or adapt aids, braces, and exercises to meet her changing needs. Too little or too much bracing can hold the child back or create new disabilities.
- Be sure crutches do not press hard under the arms; this can cause paralysis of the hands.
- Try not to let the child’s physical disability hold back her overall physical, mental, and social development. Provide opportunities for her to lead an active life and take part in games, activities, school, and work with other children.
“WILL MY CHILD EVER BE ABLE TO WALK?”
This is often one of the first questions asked by the parents of a disabled child. It is an important question. However, we must help parents realize that other things in life can be more important than walking.
If the child whose legs are severely paralyzed by polio is to walk, generally she will need at least 2 things:
-
fairly strong shoulders and arms for crutch use
- fairly straight legs (hips, knees, and feet). (It is important to correct contractures so that the legs are straight or nearly straight before trying to adapt braces for walking.)
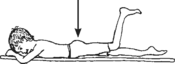
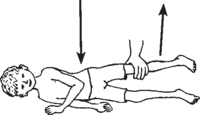
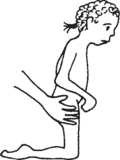
To evaluate a child’s possibility for walking, always test arm and shoulder strength:
Have her try to lift her body weight off the ground with her arms, like this:
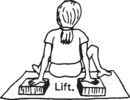 |
If she can easily lift up and down several limes, she has a GOOD chance of being able to walk using crutches. If her arms and shoulders are so weak she cannot begin to lift herself, her chances for crutch-walking are POOR. |
If her shoulder and arm strength is FAIR, and the child can almost lift herself, daily exercise lifting her weight like this may increase strength enough to make crutch use possible.
| Having the child lift herself while holding a bar like this will also help strengthen her hands and wrists for crutch use. | 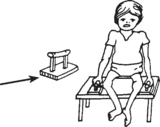 |
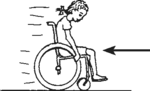 |
Pushing herself in a wheelchair or wheelboard (trolley) is a practical way to strengthen shoulders, arms, and hands. |
 |
If the child cannot lift herself because of weak elbows, put simple splints on her arms to see if she can lift herself with these. | If she can lift herself with the elbow splints, maybe she can use crutches that give elbow support. |
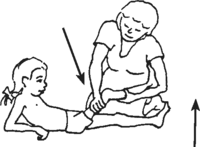
Now check how straight the legs will go.
| If the hips, knees, and feet can be placed in fairly straight positions, chances for walking soon with braces are good (if arm strength is good). | But if the child has much contracture of the hips, knees, or feet, these will need to be straightened before she will be able to walk. | |
 |
 |
|
| For correction of contractures, see Chapters 8 and Chapter 59. |
| Sometimes, if contractures are severe in one leg only, the child can learn to walk on the other leg only, with crutches. But it is best with both legs, whenever possible. | 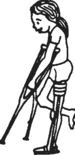 |
After checking arm strength and leg straightness, the next thing to check is the strength in the ankles, knees, and hips. This will help you decide if the child needs braces, and what kind.
A child with a foot that hangs down (foot drop), or flops to one side may be helped by a below-knee brace of plastic or metal.
 |
Foot drop: he cannot lift his foot |  |
Foot flops to one side. |  |
| PLASTIC | METAL |
 |
 |
For foot drop, you can make a brace that lifts the foot with a spring or rubber band.
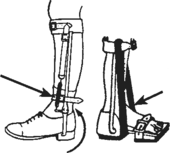 spring
joint
piece of inner tube
|
The kind of brace you choose will depend on various factors, including cost, available skills and materials, and what seems to work best for the particular child. Advantages and disadvantages of different kinds of braces, and how to make them, are discussed in Chapter 58.
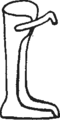
A child with a weak knee may need a long-leg brace of plastic or metal.
 cannot lift
cannot lift
weak thigh and lower leg muscles |
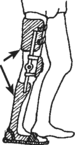 plastic |
 metal |
Upper-leg braces may be made with or without a knee joint that locks straight for walking and bends for sitting. Different models are discussed in Chapter 58. |
Note: Not all children with knee weakness need long-leg braces. A child with strong butt muscles may be able to walk without a brace.
| strong butt muscles | STRONG butt muscles pull the thigh back and keep the knee from bending. | 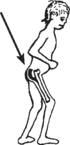
|
 |
| A child who has FAIR butt strength and a straight knee may be helped enough by a lower-leg brace that pushes the knee back. | 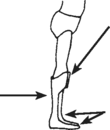 |
brace pushes knee back Slightly downward angle of a stiff brace causes it to push the knee backward when weight bearing. |
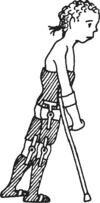
| A child with weak butt muscles may walk with one hand pushing on the weak thigh. | 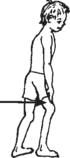 |
Or he may walk by bending the knee back to ‘lock’ it for weight bearing. | 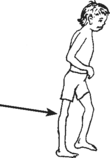 |
If a child has a contracture and cannot walk with his knee straight, correcting the contracture until his knee bends very slightly backward may allow him to walk better.
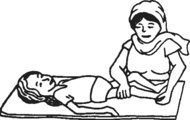
A child with very weak hip muscles may find his leg flops or twists about too much
with a long-leg brace.
| If muscles are weak here | the child cannot lift like this | ||
 |
|||
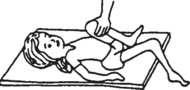
 |
or if he cannot turn his leg in and out like this, | it may flop and twist with a brace like this | 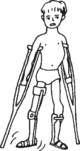 |
He may need a brace with a hip band to help stabilize the leg at the hip.
| A hip band that sits on the butt often provides better posture than a higher waistband. joint for sitting (with a lock if necessary) |
 |
A hip band that passes above the butt often lets the butt stick way out and causes swayback. | 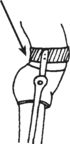 |
| A plastic hip band is less stable but more flexible and allows better stepping in some children. | |||
| BETTER | WORSE | ||
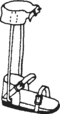
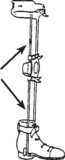
A child with weak body and back muscles, who cannot hold up her body well, may need long-leg braces attached to a body brace or body jacket.
 If she has difficulty holding her body up like this ...
|
 ... she may need a brace with body support.
|
Note: Often a child at first may need a hip band or body jacket to help stabilize her for walking. A few weeks or months later she may no longer need it. Removing it may help the child gain more strength and control. It is important to re-evaluate the child’s needs for bracing periodically.
Take care to use no more bracing than is needed.
 |
A child whose backbone is becoming seriously curved may benefit from a body brace (or in severe cases, she may need surgery). If necessary, the body brace can be attached to long-leg braces as shown above. |
 |
More information on spinal curve can be found in Chapter 20. For information on how to make body braces and jackets, see Chapter 58.