

Hesperian Health Guides
Evaluating the Progress of the Whole Child
HealthWiki > Disabled Village Children > Chapter 5: Simple Ways to Measure and Record a Child’s Progress > Evaluating the Progress of the Whole Child
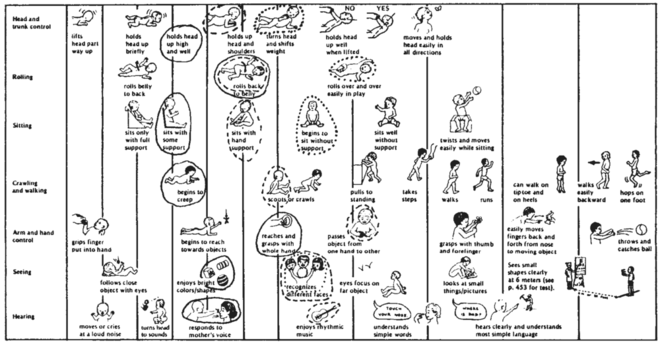
For children under 5 years old, one way of evaluating a child’s development is to use the RECORD SHEET 6. This chart shows the developmental levels (‘milestones’) for different skills and activities. The first time the child is evaluated, circle the drawing that shows what the child can do in each area.
Each time the child is evaluated, on the same sheet, again circle the appropriate drawing, but use a different color (or a dotted, dashed, or zigzag line). This way, you can see where the child is moving ahead well and where he is behind.
For evaluating the progress of children over age 5, the charts below may help. Two different approaches are used. Chart A is more objective (requires less personal judgment or opinion) but does not allow for small improvements. Chart B is more subjective (is based more on personal judgments). It considers quality of improvement, not just quantity. You can try both and see which you think gives truer, more useful results.
To use Chart A: For each skill, circle whether the child can do it “without help,” “with a little help,” or “with lots of help.” Add all the numbers you circle. Compare the scores of the first and second visits. For example:
| First visit | Second visit | |||||
| without help | little help | lots of help | without help | little help | lots of help | |
| How does the child eat? | 4 | ➁ | 0 | ➃ | 2 | 0 |
| How does the child drink? | 4 | ➁ | 0 | 4 | ➁ | 0 |
Note: We question whether the use of numbers may not be misleading. But we think the questions themselves may be a useful guideline. None of these evaluation forms will show all areas of change or improvement. They are not substitutes for detailed notes, drawings, and a good memory!
Click here for PDF of the following chart
| EVALUATION OF PROGRESS—CHILD OVER AGE 5 | ||||||
| Name______________________________________ Age_______ Disability_______________ | ||||||
| CHART A | First visit____________ (date) | Second visit____________ (date) | ||||
| Daily activities | without help | little help | lots of help | without help | little help | lots of help |
| Feeding | ||||||
| 1. How does the child eat? | 4 | 2 | 0 | 4 | 2 | 0 |
| 2. How does the child drink? | 4 | 2 | 0 | 4 | 2 | 0 |
| Dressing and washing | ||||||
| 3. Does child wash face and body? | 4 | 2 | 0 | 4 | 2 | 0 |
| 4. Does child dress? | 4 | 2 | 0 | 4 | 2 | 0 |
| 5. Does child put on orthopedic equipment? | 4 | 2 | 0 | 4 | 2 | 0 |
| Bowel and bladder care and control | ||||||
| 6. Does child stay clean (bowel control)? | 4 | 2 | 0 | 4 | 2 | 0 |
| 7. Does child clean herself after shitting? | 4 | 2 | 0 | 4 | 2 | 0 |
| 8. Does child stay dry during the day? | 4 | 2 | 0 | 4 | 2 | 0 |
| 9. Does child stay dry at night? | 4 | 2 | 0 | 4 | 2 | 0 |
| Mobility/transfers | ||||||
| 10. Does child move from chair to bed and back? | 4 | 2 | 0 | 4 | 2 | 0 |
| 11. Does child move from floor to bed and back? | 4 | 2 | 0 | 4 | 2 | 0 |
| Movement | ||||||
| 12. Walks on flat surface? | 4 | 2 | 0 | 4 | 2 | 0 |
| 13. Walks on uneven surface? | 4 | 2 | 0 | 4 | 2 | 0 |
| 14. Climbs up and down stairs? | 4 | 2 | 0 | 4 | 2 | 0 |
| 15. Uses a wheelboard or wheelchair? | 4 | 2 | 0 | 4 | 2 | 0 |
| 16. Does child crawl? | 4 | 2 | 0 | 4 | 2 | 0 |
| Social activities/communication | ||||||
| 17. Does child help with housework or farm work? | 4 | 2 | 0 | 4 | 2 | 0 |
| 18. Does child play with other children? | 4 | 2 | 0 | 4 | 2 | 0 |
| 19. Does child go to school? | 4 | 2 | 0 | 4 | 2 | 0 |
| 20. Does child speak? | 4 | 2 | 0 | 4 | 2 | 0 |
| 21. Does child communicate with signs or gestures? | 4 | 2 | 0 | 4 | 2 | 0 |
| Total _________ | Total _________ | |||||
| CHART B | First visit | Second visit | ||||
| Quality of activities | make notes for comparison here | much better | a little better | same | worse | |
| Does child move about better? | 4 | 2 | 0 | -4 | ||
| Does he sit in a better position? | 4 | 2 | 0 | -4 | ||
| Does he walk better (straighter, with less limp, or with less support)? | 4 | 2 | 0 | -4 | ||
| Does he walk farther, faster, or easier? | 4 | 2 | 0 | -4 | ||
| Are his joints straighter (less contractures)? | 4 | 2 | 0 | -4 | ||
| hip? | 4 | 2 | 0 | -4 | ||
| knee? | 4 | 2 | 0 | -4 | ||
| ankle? | 4 | 2 | 0 | -4 | ||
| Can the child do things he could not do before? | 4 | 2 | 0 | -4 | ||
| feeding? | 4 | 2 | 0 | -4 | ||
| bathing? | 4 | 2 | 0 | -4 | ||
| dressing? | 4 | 2 | 0 | -4 | ||
| toileting? | 4 | 2 | 0 | -4 | ||
| Does he play with things better? | 4 | 2 | 0 | -4 | ||
| Does he speak or communicate better? | 4 | 2 | 0 | -4 | ||
| Does he get along with other children better? | 4 | 2 | 0 | -4 | ||
| Does he seem happier or more self-confident? | 4 | 2 | 0 | -4 | ||
| Has he improved or got worse in other ways? | 4 | 2 | 0 | -4 | ||
| In what ways? | ||||||
| Total _________ | ||||||