

Hesperian Health Guides
Successful Feeding Involves the Whole Child
HealthWiki > Disabled Village Children > Chapter 36: Feeding > Successful Feeding Involves the Whole Child
It is not enough simply to put food or pour drink into the mouth of a child who has difficulty sucking, eating, and drinking. First, we must look for ways to help the child learn to suck, swallow, eat, and drink more effectively. Here are some suggestions.
POSITIONS FOR FEEDING
Positions for breastfeeding
Be sure the child is in a good position before you begin feeding her. The position will make feeding either easier and safer, or more difficult and unsafe.
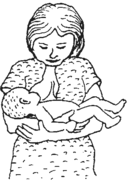
| Do not feed the baby while she is lying on her back because this increases the chance of choking. In a child with cerebral palsy, it often causes backward stiffening, and makes sucking and swallowing more difficult. |
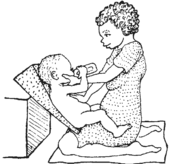
Feed the baby in a half sitting position with her head bent slightly forward. In a child with cerebral palsy, to keep the head from pushing back, hold the shoulders forward, keep the hips bent, and push firmly on the chest. |
Do not let the head tilt backward. It makes swallowing harder and may cause choking. In a child with cerebral palsy, avoid pushing the head forward like this. It will cause the baby to push her head back more forcefully. |
 |
 |
 |
| WRONG | RIGHT | WRONG |
Positions for feeding with a bottle, spoon, or finger are like those for breast feeding.
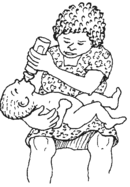
| If the baby does not suck and swallow well, the mother may think she should put a bigger hole in the nipple, tilt the baby’s head back, and pour the milk into the baby’s mouth. | Position the baby so that the head is slightly forward, and the bottle comes from in front, not above. Pushing gently on the chest helps stop backward stiffening so the baby can swallow better. |
To avoid the backward stiffening, bend the shoulders and back forward, keeping the hips and knees bent. Be sure the head bends a little forward. |
| WRONG | RIGHT | RIGHT |
 |
 |
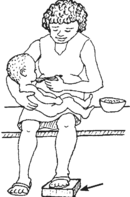 foot lift to keep the baby’s knees higher |
| But this may choke him, and it does not help him learn to suck well. | If possible, have baby hold bottle. | Place food below and in front of child, not above or behind him. |
| REMEMBER: When feeding a child with cerebral palsy, giving food from above often causes the head to press back and body to stiffen. It makes swallowing difficult. | 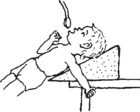 WRONG |
| Giving food from in front helps stop stiffness and makes eating and swallowing easier. | 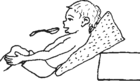 RIGHT |
 |
 |
 |
Bend flaps out some (heat to bend if necessary). |
See other seating ideas.
HELPING CONTROL MOUTH FUNCTION
The child may also need help in improving the sucking-swallowing reflex, and her ability to eat from a hand or spoon and to drink from a cup. Sometimes these can be improved by using what is called jaw control.
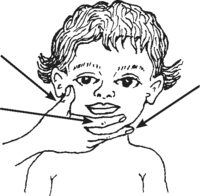
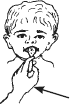
Jaw control. Before giving the breast, bottle, spoon or cup, place your hand over the child’s jaw, like this:
| if you sit beside the child | if the child is facing you | |
 thumb over jaw joint
index finger under lip |
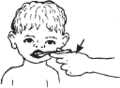
middle finger placed firmly under chin (Gently and firmly pushing the chin up is the most important part of jaw control.) | 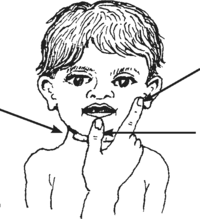 index finger over jaw joint
thumb between chin and lower lip |
At first the child may push against your hand, but after she gets used to it, it should help her control the movement of her mouth and tongue. Be sure not to push her head back, but keep it bent forward slightly.
While you feed the child, apply gentle, firm steady pressure—not off and on. Good positioning together with jaw control will help with several challenges common in cerebral palsy, such as pushing the tongue forward, choking, and drooling (dribbling). As mouth control improves, gradually lessen and finally stop jaw control.
For more suggestions for controlling drooling and improving use of the lips and tongue, see the section on developing speech.
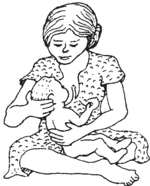
| For the child who has difficulty breast feeding (or bottle feeding), as you apply jaw control try bringing her cheeks forward with your fingers. | If you bottle-feed the baby, a large round nipple usually works best. If the child still has trouble sucking, try making the hole in the nipple bigger and thickening the milk with corn meal, gelatin, or mashed food. |
|
| At the same time, push gently against the child’s chest with your wrist. (This may help the child who tends to stiffen backward.) | 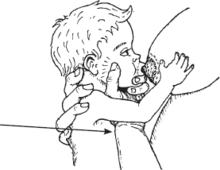 |
 |
Spoon feeding
The child who has no sucking-swallowing reflex needs to be fed with a spoon.
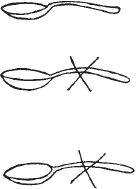
Always give the spoon from in front, |
 not from the side. |
 and not from above. |
| RIGHT | WRONG | WRONG |
Tongue thrusting
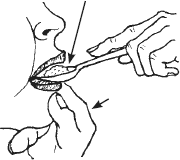
A baby sucks by moving her tongue forward and backward. For this reason, when the child begins to eat from a spoon, her tongue will at first push part of the food out of her mouth. She has to learn to use her tongue differently—pushing the food between the gums to chew, and to the back of her mouth to swallow. Children with developmental delay or cerebral palsy may have trouble learning to do this, and continue to push or “thrust” the tongue forward for some time. Do not mistake this for meaning she does not like the food.
Jaw control, although helpful, may not be enough to prevent this tongue thrusting. It also helps to apply firm pressure with the back of the spoon on the tongue as you feed the child. This helps keep the tongue from pushing forward and lets the child use his lips and tongue better.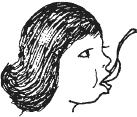
Do NOT scrape the food onto the upper lip or teeth as you take the spoon out. Instead, let the child try to get the food off the spoon onto her tongue. To make it easier for her, start by putting only a little food on the end of the spoon. as you take the spoon out, make sure the mouth is closed so that the tongue can move the food inside the mouth and cannot push it out.
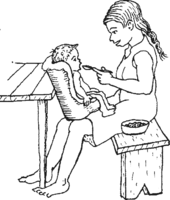
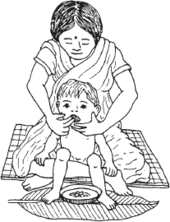
If eating with fingers is the custom, or if spoon feeding is too difficult, use your fingers.
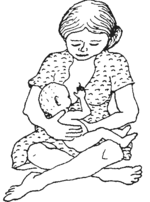
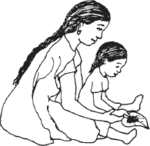
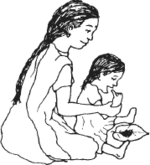
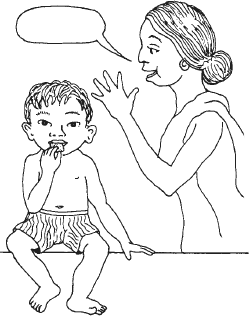
| Here a mother holds her child in a good position on her lap, using her legs and body to give support. With one hand she gives jaw control while she feeds him with the fingers of the other hand. Place a little food on the side or middle of the tongue—not on the front of it. |
 |
For spoon or finger feeding, it is best to start off with soft, mushy foods rather than liquids. Milk (even breast milk) or egg yolk can be mixed with rice paste, boiled corn, or mashed beans. You can also give small pieces of fruit, mashed greens and vegetables, and yogurt or soft cheese. Hardest for the child to eat are combinations of liquids and solids—such as vegetable soup. |
Chewing
To help the child learn to chew, put a bit of firm food in the side of her mouth between her teeth. Use very small pieces of bread crust, tortilla, or chapati. Help her close her mouth using jaw control.
| Biting off can be encouraged by pulling slightly on a long thin piece of food. Or rub the piece of food against the teeth before putting it between them. | 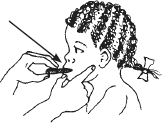 |
cord |
| A finger-shaped piece of tough cooked or dried meat or very tough chicken (old rooster) can be used instead of the cord. Be sure it is too tough for the child to chew pieces off of it, but juicy or tasty enough to give her pleasure. |
If the child has difficulty chewing and chokes on pieces of food, try this:
Cut a piece of clean, soft cotton cord, or braid thin strips of cotton cloth. Soak or cook the cord in a tasty good food and hold the end while she bites and chews on it, squeezing out the nutritious juices. Help with jaw control.
This method is completely safe. Because you hold on to the cord, the child cannot bite off pieces and choke on them. It is best to practice this at the beginning of a meal while the child is still hungry.
|
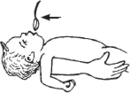
CAUTION! If a piece of food slips back into the child’s throat and gets stuck, bend the child far forward, and keep calm. The food should drop out. Do NOT pat the child on the back as this could cause the child to breathe in the food.
|
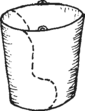
Drinking
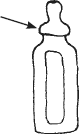
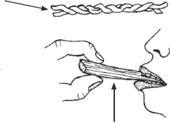
| You can make a special cup from a plastic bottle. |  |
| Cut it like this. |  |
| Gently heat the rim and gradually bend it out with a round smooth rod or stick. | 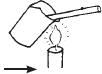 |
| Successful drinking, like eating, involves the whole child. Body position is important. For example, in a child with cerebral palsy, to drink from a regular cup or glass, his head must be tilted back. But this can cause uncontrolled backward stiffening and possible choking. | 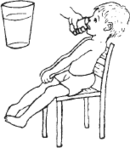 |
| However, if he uses a plastic cup with a piece cut out, he can drink without bending his head back. | |
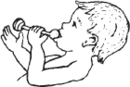
| The cup should have a projecting rim. |  |
Cut out a space to fit around the child’s nose. |  |
| This way the child can drink in a better, more controlled position. | 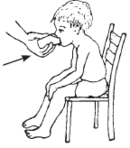 | ||
At first you may need to apply jaw control to help the child close her lips on the rim of the cup. Tilt the cup so that the liquid touches the upper lip and let the child do the rest. Do not take away the cup after each swallow as this may trigger pushing the head back or tongue out. It helps to start with thick liquids—like cooked cereals, maize mush, or yogurt.
Self-feeding
To be able to feed herself, a child needs more than control of her mouth, lips, and tongue. She also needs to be able to sit with her head up, to pick things up, and to take them to her mouth.
To prepare for self-feeding, encourage the child to play, taking his hands and toys to his mouth. Also, encourage him, when sitting, to balance while he uses both hands (see "Helping improve balance" and "Activities for Body Control, Balance, and Sitting").
A child who has difficulty with balance or uncontrolled movements will at first need special seating adapted to her needs.
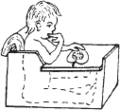
| A HIGH CHAIR | A CARDBOARD BOX SEAT | 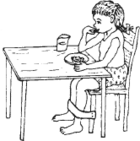 |
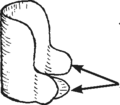
Some children with cerebral palsy may only need a foot strap to stay in a good position (to keep the body from straightening stiffly as shown above). | |
| Try one or more straps, to see what works best. | 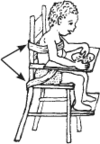 |
 |
||
When a child is delayed in using her hands to grasp things, or to take things to her mouth, you can help her discover how to use her hands and feed herself, like this:
| Put the child’s finger in a food she especially likes. | Then lift her finger to her mouth. | Help her to do more and more, step by step, until she does it alone. |
 |
 |
 |
Little by little help her less and less. Lift her hand to her mouth and touch her lips with the food. See if she will then put it into her mouth. When she has learned this, lift her hand near her mouth and see if she will do the rest. Next just put her finger in the food and encourage her to lift it to her mouth. Each time she does more for herself, praise her warmly.
This method is part of a behavioral approach to teaching new skills. The same approach can be used for teaching the child many skills related to eating, such as using a spoon or drinking from a glass. To learn more about this approach, see Chapter 40, “Ways to Improve Learning and Behavior.”
| A cover or bib like this, of plastic or waterproof cloth, is a big help. The pocket at the bottom catches spilled food. | 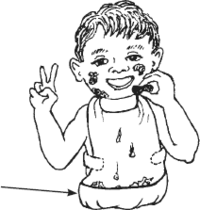 |
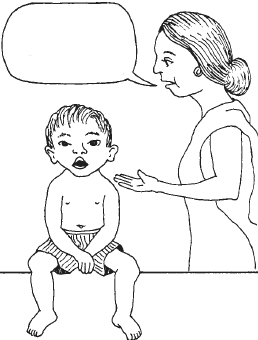
While it is important not to push or hurry children too much in developing feeding skills, the opposite is also true. Often parents wait too long and do not expect enough from their child with disabilities. Below. see how a rehabilitation worker helps parents awaken to the ability of their child with cognitive delay to learn new skills.
THE 6 MINUTE BISCUIT TRICK FOR DEVELOPMENTALLY DELAYED CHILDREN
by Christine Miles of Peshawar, Pakistan, and Birmingham, United Kingdom
Here is how I get parents to open their eyes to what their child actually can do and learn to do. I see many parents with developmentally delayed children between 15 and 30 months. They have realized that the child is not functioning at a level appropriate for his age. But often they cannot describe what the child actually can do, and do not seem to realize that children gain new skills by learning. Parents complain that “He doesn’t speak. He can’t do this, he can’t do that,” as though there is something wrong with the machinery or someone has failed to push the correct button.
I ask them whether the child can eat a biscuit (cookie). “No, he only has milk and mush. He can’t feed himself.” I get a biscuit and put it into the child’s hand. I guide the hand up to the mouth. Sometimes the child will bite on the biscuit; sometimes it needs to be tapped gently against his teeth and wetted with his lips and tongue until a piece breaks off and is eaten. I move the child’s hand away from the mouth, then repeat the process. Usually by the time half the biscuit has gone, the child has learned how to do it, and finishes the biscuit happily without help. The parents usually say “Oooh!”
In 6 minutes the parents have watched their child learn an important skill, by our using a simple directed action and a strong reward (tasty food). No matter how developmentally delayed their child is, the parents gain some vital information about the child’s ability to learn. Whether or not they remember anything else that I say to them, they go away with a whole new experience to think about. almost always they have consulted several doctors before coming here, without gaining any useful advice.
Of course, it is not guaranteed to work. But it does work surprisingly often. The 6 minute biscuit trick is a powerful stimulant to parents to actually observe their child and to help the child learn.