Hesperian Health Guides
Doing the MVA
-
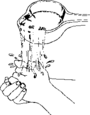
Create a vacuum in the syringe:
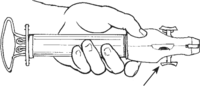 Push the button inward and forward.
Push the button inward and forward.
Hold the barrel of the syringe with one hand and pull the plunger back with the other hand, until the arms of the plunger snap outward at the end of the syringe
With the plunger all the way into the cylinder, close the valve by pushing the button inward and forward — the button will make a “click” sound and will stay stuck in place until you open it again.barrel.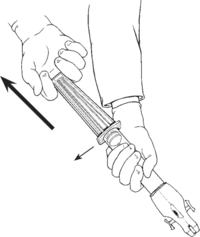 Pull the plunger back.The arms of the syringe will snap out.
Pull the plunger back.The arms of the syringe will snap out.
Check the arms of the plunger. They should both be out as far as they can go. With the arms snapped in this position, you should not be able to push the plunger back into the barrel. - Shine a light on the woman’s genitals so you can see well. You may need a helper to hold the light.
- Wash your hands with soap and water for several minutes. Let your hands dry in the air. Put clean plastic gloves on your hands.
- When the woman tells you she is ready, follow the steps for a bimanual exam. Feel the size of the womb. The womb should be the right size for the number of weeks the woman has told you that she was pregnant. If her womb is very big, she might have been pregnant for longer than she thinks. Do not do MVA for a woman who is more than 3 months pregnant, unless she is having serious problems from an incomplete abortion and you have no other way to help her.
- Take off your gloves, wash your hands, and put on new, sterile gloves. This will allow you to keep all the tools for the MVA sterile as you do the procedure.
-
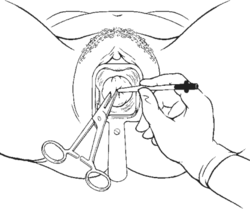
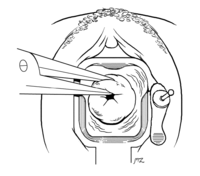
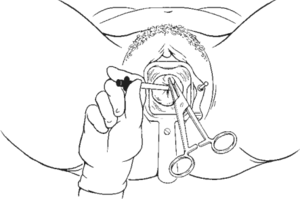
Gently insert a speculum.
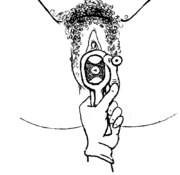
- Dip a piece of sterile gauze held with the ring forceps,or a long swab, into antiseptic. Use the gauze or swab to wash the cervix.
-
If you have decided to give an injection to numb the cervix, do so now.</span</li>
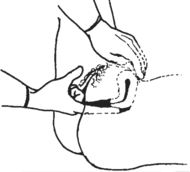
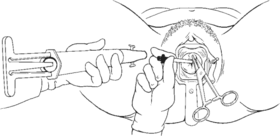
- Ask the woman to breathe deeply and relax. When she is ready, grasp the cervix with a tenaculum or a ring forceps. Close the tenaculum and pull it a little to straighten the womb. This can be very uncomfortable for the woman, so be gentle and tell her what you are doing.
Injections to numb the cervix

You will need a sterilized 3 cm (1 inch) needle and 20 ml of 1% lidocaine or another local anesthetic with no epinephrine in it.
Before the injection, ask the woman if she has had this kind of anesthetic medicine before. Find out if she ever had a bad reaction to this medicine. If she has had a bad reaction, do not give the injections.
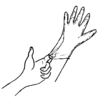
Follow the instructions to prepare and give an injection. For these injections, you will insert the needle about 1 centimeter under the skin and inject slowly as you pull the needle out.
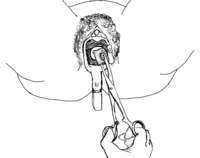
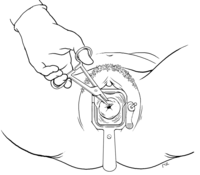
After placing the speculum and using antiseptic to wash the cervix, inject 2 ml of lidocaine at the top of the cervix (12 o’clock) where you will later grasp with the tenaculum. Then grasp the cervix with the tenaculum, and use it to move the cervix a little to the side until you can see the place where the cervix (which is smooth) joins the vagina (which is more rough). Then give 4 injections of the rest of the lidocaine where the cervix joins the vagina, at 2, 4, 8 and 10 o’clock.
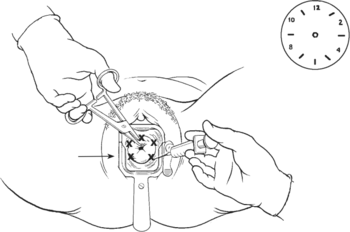 Inject the medicine into these spots.
Inject the medicine into these spots.
You can now begin the MVA. The woman may still feel cramping after the injection, but it will not hurt as much.
- Ask the woman to breathe deeply and relax. When she is ready, grasp the cervix with a tenaculum or a ring forceps. Close the tenaculum and pull it a little to straighten the womb. This can be very uncomfortable for the woman, so be gentle and tell her what you are doing.
-
Choose a cannula. Cannulas come in many different sizes (the size may be printed on it). The larger a woman’s womb is, the larger a cannula you should use. This chart gives you an idea of which cannula might work best:
For a woman who is
5 to 7 weeks pregnant
(9 cm long womb) use a 5 mm cannula
use a 5 mm cannula7 to 9 weeks pregnant
(10 cm long womb) use a 6 mm cannula
use a 6 mm cannula9 to 12 weeks pregnant
(12 cm long womb) use a 7, 8, 9, 10, or 12 mm cannula
use a 7, 8, 9, 10, or 12 mm cannula - Some types of cannula need an adapter to fit onto some syringes. If you need an adapter, attach one now.
- Tell the woman that you are ready to start. When she is ready, gently push the sterilized cannula through the opening in the cervix. Do not let the cannula touch anything — even the walls of the vagina — before it goes into the cervix. Sometimes the cervix is too tight to let a large cannula in. If this is the case, first insert a small cannula into the cervix, and then take it out and put in a larger cannula.
Try gently turning the cannula as it passes through the cervix. This will make it easier to insert. As you insert a cannula, pay attention to the woman to make sure she is not in pain. Ask her to tell you if the procedure hurts. Sometimes the expression on a woman’s face will tell you she is in pain even though she is not making any sounds.
If the woman is in pain, slow down. Moving slowly will help prevent injuries. Ask the woman to take deep breaths to help her relax and to help her cervix open. -
Gently guide the cannula in until you feel it stop at the top of the womb. When you feel the top of the womb, pull the cannula back just a little. If you need to, you can let go of the tenaculum.
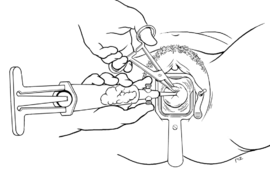
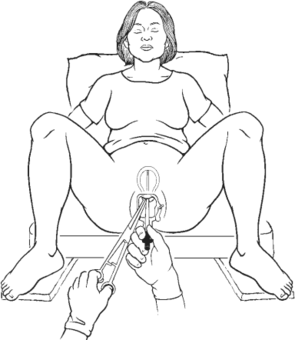
- Hold the syringe with one hand and the cannula with the other. Attach the syringe to the cannula by pulling the cannula slightly back onto the syringe. Make sure you do not push the cannula forward into the womb. Pushing too far will injure the womb.
- Pinch the button on the syringe toward yourself to open the valve. The button will make a clicking sound. Foamy and bubbly fluid and some blood and tissue from the pregnancy will flow from the womb into the syringe. Some blood may also come out into the vagina.
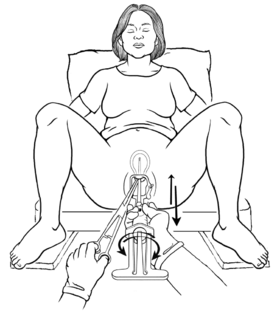
- Empty the womb by slowly and gently moving the cannula in and out while you rotate the syringe. Do not pull the tip of the cannula out of the womb If you pull the cannula tip out of the cervix, the vacuum will be broken. Even if you push the cannula back into the womb, it will not pull tissue anymore. The MVA will not be complete. Do not push the cannula too far in or you could injure the womb.
-
Keep moving and turning the syringe until the womb is empty. Usually, the womb empties within 5 minutes.
These are the signs that the womb is empty:
- There is only pinkish foam in the cannula.
- There is no more tissue in the cannula.
- When you touch the cannula tip to the inside of the womb, it feels rough and gritty.
- The womb tightens down and “grips” the cannula.
-
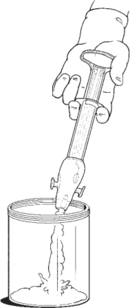
When the womb is empty, take the syringe off the cannula. Empty the syringe into a clear container, like a glass jar.
Now gently pull out the cannula, and then remove the tenaculum and take out the speculum.
- Look at the tissue from the womb to see if it is complete. It is important to know if you have removed all the tissue, because if any is left inside the womb it can cause infection and bleeding
Pour the tissue through a sieve or add some clean water to the jar it is in. What you see will depend on why the woman needed the MVA.If the woman had an MVA to end a pregnancy or because she was bleeding from a miscarriage, you should see the complete pregnancy. After 4 weeks of pregnancy, there should be white or yellowish feathery tissue attached to a small, clear sac. If you do not see all this material, repeat the MVA.
If you are doing an MVA to empty the womb after an incomplete abortion or incomplete miscarriage, you might not see all of this tissue. Some of it may have already passed out of the womb. Take note of what you see anyway. If you did not see the complete pregnancy tissue when you did the MVA, and the woman has bleeding or signs of infection later, you should repeat the procedure.
- Safely dispose of the bloody tissue.
WARNING! Never squeeze the arms of the plunger together or push the plunger into the barrel while doing an MVA. That would push the contents of the syringe back up into the woman’s womb. This could kill the woman.